Subscribe on Google | Apple Podcasts | Spotify | Amazon
In nursing school, Norah Lusk already knew she wanted to work with sexual assault survivors. She had seen how this part of the health care system was “sorely lacking” through victim-blaming, long wait times and a shortage of specialized practitioners.
Now a sexual assault nurse examiner, or SANE, Lusk is trained to care for survivors of violence. SANEs conduct forensic exams, collect evidence, provide follow-up care, advise survivors on their reporting options, testify at trials and more.
Lusk works in an emergency room in Elko, Nevada − a four-hour drive from Reno. In between the two cities, there is nowhere for sexual assault survivors to receive forensic exams, which are essential for law enforcement investigations.
Survivors in Lusk’s area might have to travel hundreds of miles for proper medical care. The burden is often on them to know where to go and how to get there − all after experiencing a major trauma.
“There’s a victim population that is not being served at all,” Lusk said.
Across the U.S., forensic nurses are equally scarce.
“Nobody really knows where SANE exams are available,” said Leah Griffin, a sexual assault advocate and survivor who, in 2014, was turned away from a Seattle hospital that did not provide forensic exams.
Despite a 2022 law requiring a national directory of sexual assault nurse examiner locations, there is no comprehensive national resource to direct survivors to the nearest forensic exam. Congress tasked the Agency for Healthcare Research and Quality to create the resource but did not allocate funding for the project, leaving the agency unable to create it.
Though more than half of states have their own SANE databases, some are incomplete or outdated − out of 30 databases, eight haven’t been updated in a year or more. Twenty states do not have directories for post-assault medical care at all.
“If you’ve experienced violence, I guess you’re just supposed to know what to do,” said Jennifer Johnson, president and co-founder of the Academy of Forensic Nursing. “And I think that’s a cop-out.”

Obstacles to care
The Rape, Abuse and Incest National Network estimates that someone is sexually assaulted in the U.S. every 68 seconds. Medical care afterward is key to addressing physical and mental health needs and collecting evidence.
Forensic exams − commonly known as rape kits − are voluntary and required by federal law to be free. Depending on patient need and consent, the exam can include urgent medical treatment, a full body examination, DNA collection and photographic documentation.
Forensic nurses provide more comprehensive care and more accurate evidence collection than other medical staff, according to the U.S. Department of Justice’s Office for Victims of Crime. SANE involvement also increases sexual assault reporting rates, the number of charges filed, conviction rates and the average sentence times for offenders.
Regardless of whether a survivor wants to involve law enforcement, forensic exams influence health outcomes by testing for pregnancies and sexually transmitted diseases. SANEs also evaluate patients’ psychological states and connect them to mental health resources and advocacy groups for long-term support.
Registered nurses can receive SANE training from universities, state agencies and professional organizations like the International Association of Forensic Nurses. This specialized education focuses on conducting forensic exams and interviews, providing trauma-informed care and working with law enforcement.
But only about 1 in 5 U.S. hospitals have a SANE available, according to IAFN. And providing 24/7 coverage “can be a real challenge,” Johnson said. The problem is even worse in rural areas, like the expansive Nevada region where Lusk works.
Forensic nurse numbers have decreased in the past few years, mirroring a general post-pandemic nursing shortage. Totaling 4,500 in 2018, IAFN’s membership rose to almost 6,100 over the next two years before falling to 5,600 in 2022.
Multiple factors drive the SANE shortage, including inability to find the budget to add staff. The stress of the job also causes many to leave the profession.
“If you live in a community where the hospital doesn’t have a sexual assault program, the ultimate question is, ‘Well, then what happens?’” Johnson said.
When a survivor goes to a hospital that doesn’t have a forensic nurse examiner on staff, they typically are either told to go elsewhere or are given basic medical treatment.
While general hospital staff can administer a rape kit, Johnson said, “they’re not really trained to do the kit right.” A majority of medical and nursing school programs do not offer training on sexual assault care, according to multiple studies.
This means less evidence may be collected by general health care providers, which can affect legal outcomes. Forensic nurses also are specifically trained to testify in court about the examination, which is not typical for other hospital staff.
Even when a hospital has a SANE, the coverage may be for limited hours, which can lead to days long delays in care, Johnson said. That adds to the list of reasons survivors may not get care.
Jennifer Pierce-Weeks, CEO of the International Academy of Forensic Nurses, recounted stories of survivors traveling hours for SANE care, sometimes via costly ambulance rides. Others simply went home “because of the complexities of going to one place, not being provided care, and then trying to keep up that will to continue to seek care.”
Advocate Leah Griffin said she has spoken to survivors who were left by police at hospitals that did not provide SANE exams. Others don’t even get that far.
Phoenix resident Ron Blake said when that he was raped in 2011, he had never heard of a rape kit or a sexual assault nurse examiner. He didn’t know to go to the hospital for a forensic exam. Looking back on that night, Blake said the biggest obstacle to receiving medical care was the police.
Blake said that despite his testimony and visible injuries, none of the officers who responded to the scene offered to take him to receive medical care. Nor did anyone tell Blake where he could go to get a forensic exam.

“I did everything I was supposed to do,” Blake said. “I told the police what happened to me. They arrived, they saw all the injuries to me. It was on them. And that’s where the impediment was. That’s what stopped me from getting a forensic exam.”
Blake didn’t learn what a forensic exam was until later, when he spoke with other survivors.
“I thought: ‘Wow, what did I do wrong? Why didn’t I get that?’” he said. “It should have been an option for me, and it wasn’t.”
Blake’s case was closed with no charges. The Phoenix Police Department incident report cites the lack of a forensic exam as one of the reasons.
He now journeys across the country speaking about his experience. He has met tens of thousands of people, some of whom have opened up about their own assaults.
In situations like Blake’s, when survivors are left to search for care on their own, advocates believe a comprehensive database of SANE locations could help.
The struggle to find a provider
Last year, Congress called for a requirement to do just that.
It reauthorized the Violence Against Women Act. One section directed the Agency for Healthcare Research and Quality − part of the U.S. Department of Health and Human Services − to complete a national report on forensic exam services. It also called for the agency to create a comprehensive online map of sexual assault forensic exam availability. The entries would specify whether the forensic nurse coverage is full- or part-time.
The report and online map were set to be published no later than March 15, 2023, a year after the law’s enactment. That never happened.
The Agency for Healthcare Research and Quality did not create the resource because Congress did not appropriate funding for it, said Office of Communications Director Howard Holland. The agency did not create a cost estimate for the project, Holland said.
“If and when these activities may be included by Congress in the appropriation for AHRQ, we will take further steps to identify how we might move forward,” Holland said.
Ron Eckstein, press secretary for U.S. Sen. Dianne Feinstein, the bill’s sponsor, confirmed the mandate wasn’t funded. He said, however, that Feinstein’s office was under the impression that the database wouldn’t require additional funding to complete.
“Learning that this (resource) is held up is devastating,” advocate Leah Griffin said.
For almost a decade, Griffin has worked with lawmakers to create legislation expanding access to sexual assault nurse examiners. This included advocating for the report and SANE map.
“I fought for years for this study, so to learn now that the agency is just throwing up their hands over a miscommunication is hurtful,” Griffin said.
Without the required federal directory, other groups are trying to fill the gap.
The International Association of Forensic Nurses operates the largest national database of SANE programs. The list is updated when its members have new information. But it is neither exhaustive nor mandatory.
“It’s only as good as the data that is entered,” CEO Pierce-Weeks said. “And it’s really based on someone’s knowledge that it exists and that we’re looking for the information.”
State databases have similar shortcomings, if they exist at all, the Center for Public Integrity found.
Thirty states have online databases of SANE locations, usually maintained by advocacy groups or government agencies.
Some of these databases have connected survivors to care. Patients have reported using the Massachusetts Department of Public Health’s directory to find SANEs, said Assistant Director of Media Relations Katheleen Conti.
But other state databases are difficult to find or are outdated. The nationwide SANE shortage has forced many programs to close, and older databases may not reflect those changes.
“I see through my work that some places, especially really rural places, struggle to maintain a SANE program,” said Erin Pollitt, executive director of District of Columbia Forensic Nurse Examiners. “I would hate for somebody to see a super rural program on the (database) and immediately assume that there’s going to be a SANE there if they go.”
All 20 states without a public SANE database have lists of rape crisis centers or other support services online. Similar to RAINN’s national directory of sexual assault service providers, these resources can be helpful but do not automatically lead to medical care like a SANE database does, Johnson said.
“Every additional step that a survivor has to take, the more likely that they’re going to give up,” said Brie Franklin, executive director of the Colorado Coalition Against Sexual Assault.
Piecing together a national database would be a challenge.
In addition to inconsistent data, the requirements for SANE training and credentialing vary by state, as does who oversees the programs, Johnson said.
This means someone trying to build a database would need to coordinate with numerous offices and hope each organization has current data on where forensic nurses can be found.
A 2016 report from the U.S. Government Accountability Office found “limited nationwide data” on health care facilities with SANE programs. Out of a GAO sample of six states, only one had a formal system to track SANE locations.

More permanent solutions
The ideal solution, some advocates and practitioners say, is for every hospital to offer forensic exam services − which would make the databases unnecessary.
“I don’t want to say it’s never going to happen, but sitting here right now, it’s an open dream,” Johnson said.
A few states have tried.
In 2018, Illinois passed a law requiring every emergency room in the state to have a sexual assault nurse examiner on staff or an approved transfer plan, with no transportation costs charged to the patient. Nurses must initiate treatment within 90 minutes of the survivor’s arrival. If a hospital fails to meet the requirements, it can be fined up to $500 a day.
Hospitals were required to comply with the mandate by Jan. 1, 2023. But when asked in August whether every hospital in the state had met the requirements, Illinois Department of Public Health spokesman Mike Claffey said he didn’t know. The department is still gathering data through its hospital surveys.
Earlier this year, West Virginia’s governor signed a similar bill into law. Though the proposed legislation would have required every emergency department to have a SANE on staff at all times, a House of Delegates committee amended the bill to allow hospitals to set up a plan to transfer patients to other facilities. Unlike the Illinois law, West Virginia’s policy does not prohibit them from charging for that transport, nor does it fine hospitals that fail to comply.
“When every single hospital in the United States has trained nurses to provide medical forensic exams,” Johnson said, “then we will have enough.”
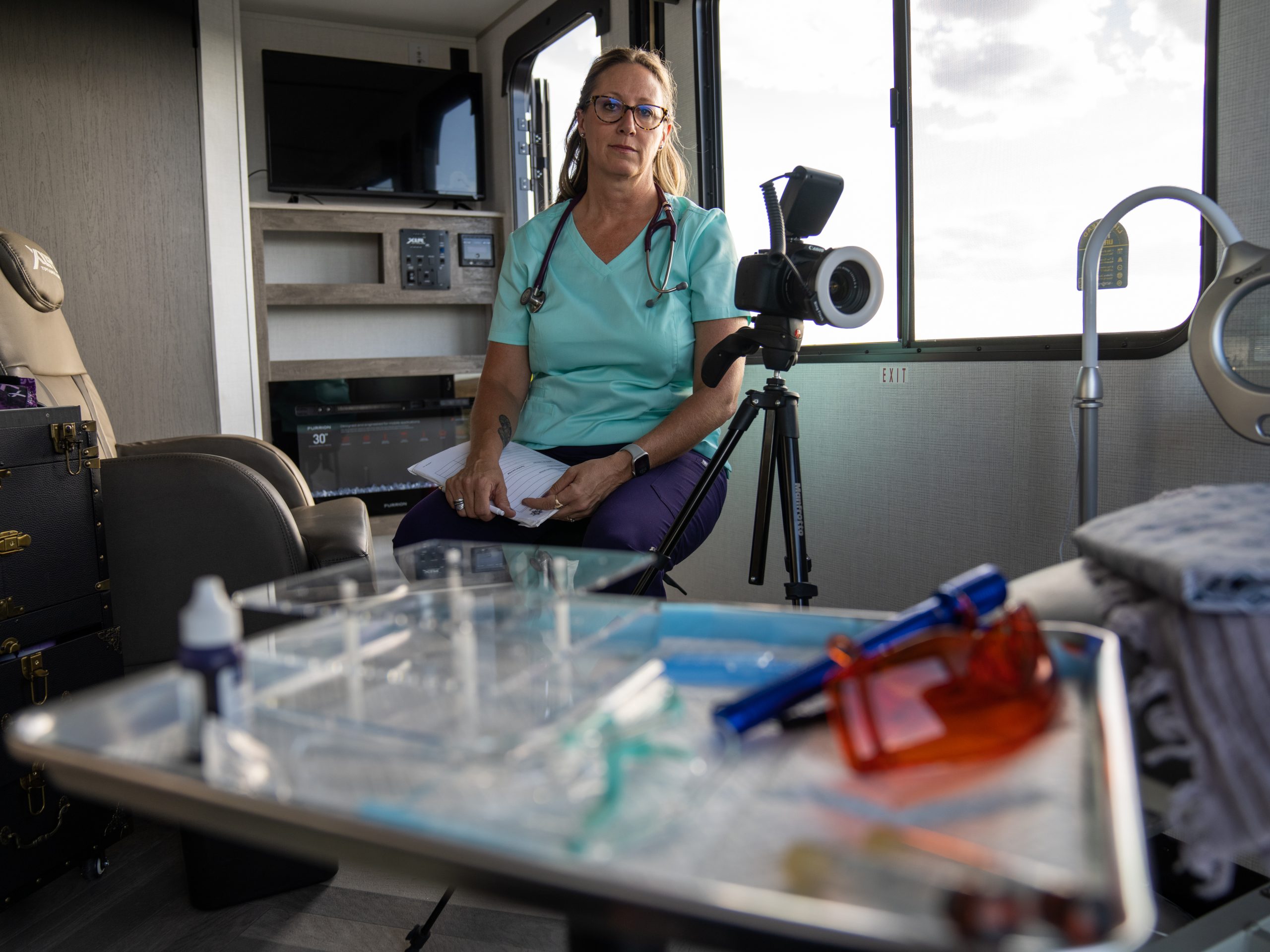
For now, some providers are working to bring nurses directly to patients in need − like Norah Lusk in Elko, Nevada.
In April 2022, Lusk and her sister-in-law created a mobile unit and called it the Nevada Institute of Forensic Nursing.
Using a travel trailer, Lusk’s team of forensic nurses, interviewers and advocates can meet survivors wherever necessary, from hospital grounds to Walmart parking lots. The vehicle is unmarked to protect patients’ privacy.
The unit is the only one of its kind in Nevada, but Lusk is working to make the institute a statewide program, with plans for a satellite office in Las Vegas. Her ultimate goal is to go national.
“If I can do this in a rural area,” she said, “there’s no reason why we can’t address this in other states.”